
Healthcare Challenge
Positive healthcare outcomes depend not only on the quality of the procedure, treatment, or drug, but also on how the service is provided to the patient. The drug may be approved, but are people taking it? The hospital may provide services, but do patients want to go there or can they go? Also, do hospitals and healthcare providers' inefficient or negative experiences prevent patients from continuing care?
These are all important questions, but in many cases there is little available funding to deal with them properly. This is because the medical and scientific research community, together with government and private funders, spends that energy on the development of medicine itself. “We are a great place to go,” said Sindy Escobar Alvarez, Director of Medical Research Program at DDF. “We also don't focus well on the study of prevention. It's best to ensure that people don't get sick in the first place.”
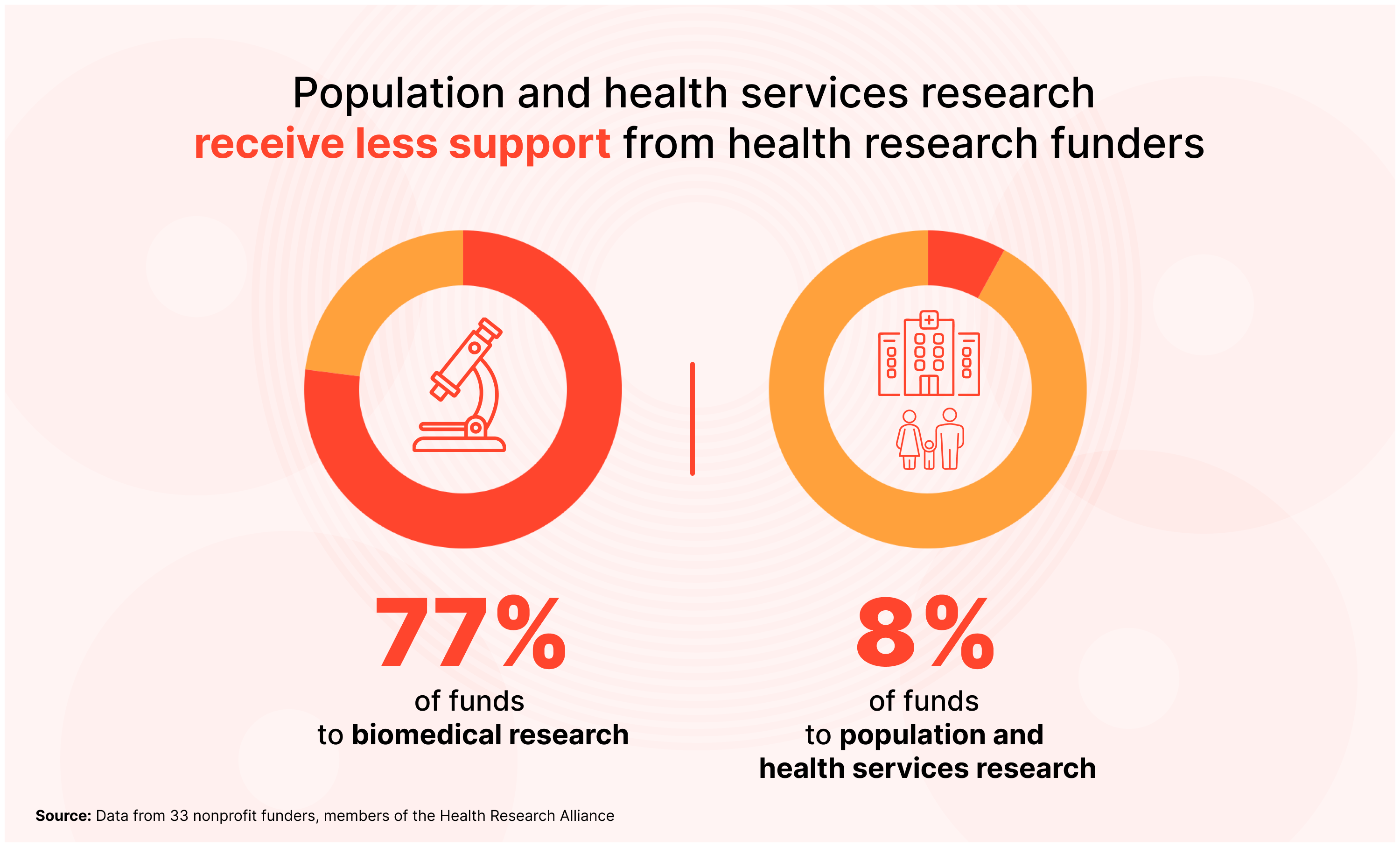
The numbers indicate cutting. Between 2012-2022, 33 nonprofit health research funders directed 77% of their funds towards biomedical research, 15% in clinical research and just 8% in population and health services research.
What is behind this challenge?
Dr. Ashwin Versan is a doctor professor of public health at Columbia University and a former New York City Health Committee physician. He has several theories as to why it is difficult to fund research that explores the challenges of providing treatment.
He says biomedical and clinical research is often carried out in “laboratory conditions.” Set to generate a hypothesis and test that hypothesis in a highly controlled setting. However, studies focusing on prevention, access and delivery can be much more difficult to control and track, especially as they rely on both quantitative metrics like statistics and qualitative metrics like in-depth interviews. These studies often need to follow the population over time. (Observation cohort studies such as nurse and physician health studies are examples.) This study may elicit associations but does not elicit causal or data regarding service delivery.
Or take research into health services, an interdisciplinary field that explores how systematic social, financial and policy reforms can improve healthcare delivery. Such research can be messy, says Dr Versan. Because you are observing the “real world state.”
This is because delivery often intersects real-time conditions in the real world, paying attention to these issues, and because funding solutions require public policy measures. This is much more complicated than funding labs or basic clinical research. And, as Dr Versan explains, the people most affected by poor healthcare tend to be underresourced communities, so people aren't always talking for them.
“We face a lot in healthcare delivery and public health, especially when it comes to reaching marginalized groups that have no natural political and social forces and voices,” says Dr. Vasan. “It hurts them when decision makers and resource allocators are deciding what is funded and what not to do. Prioritizing their prevention and care delivery needs is often an afterthought rather than a centre of the research agenda.”
Covid Vaccine: Real World Examples
Covid vaccines encapsulate much of this. As Dr Versan explains, when the Covid vaccine was first introduced, they were shown to be successful in preventing serious illness and death. However, in New York City, particularly older black Americans, did not leave their homes to receive the vaccine, despite the widespread availability and widespread support for being safe and effective.
When public health workers began studying the mechanisms of delivery, they studied how vaccines were promoted, how vaccine education was conducted, where they were administered, and who were administered. Many older black Americans, especially those who lived in public housing, did not have stable internet access and were afraid to take public transport during the pandemic. Even at local drug stores, they were not able to book or attend easily. Furthermore, research has revealed that practical and historical inequality has led to older black Americans inherently distrustful of the vaccine and the public health officials defending it. This trust barrier had to be overcome to close the gap between successful delivery and the black white vaccine.
“So the NYC Health Department designed the intervention and tested it at the same time,” Dr. Vasan said. “That's how do you reduce all the barriers to these populations getting in to access the vaccine?”
The NYC team has begun testing a new approach in real time. They began bringing vaccines to a needy population who adhered to and administered it in the culturally trusted spaces that older black Americans already had, like barbershops, churches and community centers. They worked with trusted community stakeholders, such as black doctors and pastors, to help fight misinformation. They administered home-based vaccinations for New Yorkers with limited mobility who could not physically leave the house. And they invested in local organizations (nonprofits, healthcare facilities, etc.), hired community health workers with a reliable track record of engagement and aimed at vaccine education, outreach, caring engagement, and PPE distribution and addressing basic needs.
And when all this was happening, researchers were tracking vaccination rates between communities that received this new approach and those still awaited for deployment. They conducted in-depth interviews with the target population to better understand how the new approach works.
“Our data not only showed that the program is effective, says Dr. Vasan.
Make a change
You don't have to wait to convince your funders that a public health emergency is worthy of attention. Covid is a prime example. If pre-pandemic research allowed public health officials to better understand and design interventions to address the unique challenges that older black Americans face at the centre of vaccination, they would have prepared these delivery strategies much earlier. As a result, fewer people became ill. Many people probably died. So, how do you convince a funder?
First, public health leaders like Dr Versan want funders to know that by answering real implementation questions, like how to spread vaccines, they pursue as much innovation and creativity as they would make a vaccine in the first place. “We need to raise funding habits for implementation as part of the dissemination and uptake of both proven and new prevention and care strategies,” he says. “Then you are asking the delivery question you are asking can be argued as novel and essential to the successful intervention.”
He says that even if they are not funding major clinical research, funders can link it to something that is an outdoor decision or field shift in some important way.
Third, there is a need to change the conversation about the importance of research in health services. That way, funders will understand how important it is to prevent illness and save lives. We have seen incredible scientific and medical advances, but once those drugs and treatments leave the lab or clinical research, their adoption is subject to any kind of unexpected real-world condition.
“The research community has the assumption that the best ideas will naturally be adopted, and the magnitude of their effectiveness will determine the size of the political will that will affect large-scale change,” says Dr Versant. “That's rarely the case. Policy doesn't work with magic bullets. Rather, in reality, we need a level of discernment on the part of our funders to say that this is a very important set of questions that, like the main innovation itself, is a very important set of questions that deserves support.”